Andrew Leipus in Cricinfo
Able to bowl but not throw because of shoulder pain? Or maybe you have
lost power in your throw? Have to throw side-arm? Does your whole arm go
"dead" for a few seconds after you release the ball? Or you are now
experiencing a click, crunch or clunk when you lift the arm? These are
just some of the many symptoms and behaviours that can be present in the
cricketer's shoulder and which can help clinicians diagnose what your
underlying problem might be.
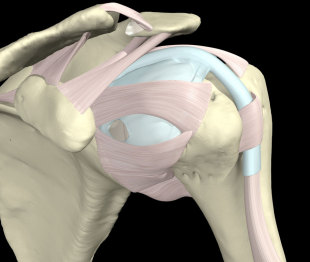
There can't be a shoulder discussion without a brief anatomy lesson. In
terms of understanding the basics, the glenohumeral joint is a shallow
ball-and-socket design, allowing a huge amount of mobility yet remaining
as stable as possible. It also has to tolerate massive torques or
rotational forces generated. Some people equate the head of the humerus
(HOH) and its relation to the scapula with a golf ball sitting on a tee,
i.e. easy to topple over. But it is actually more like trying to
balance a soccer ball on your forehead, with both the ball and the
head/body constantly moving to maintain "balance" and stop the ball from
dropping off. It is this balance between the socket joint and the
scapula position which we need to consider in the cricketer's shoulder
as it is where a lot of problems begin and where a lot of rehab
programmes fail.
As is the case with all injuries, the anatomy often lets us down by not
being able to cope with the functional demands. Some injuries develop
acutely, such as occurs with one hard throw when off balance, and some
develop over a period of time through lots of high repetition -
degenerative type injuries. The two most commonly injured structures in
cricket are the infamous rotator cuff and the glenoid labrum.
The cuff is a group of small muscles acting primarily to pull and hold
the HOH into its glenoid socket. The long head of biceps tendon assists
the rotator cuff in this role. The labrum is a circular cartilage
structure designed to "cup" or deepen this socket and provide attachment
for the biceps tendon.
An injury to the labrum results in the HOH having excess translatory
motion and not staying centred in the glenoid. The cuff then has to work
harder to compensate for this structural instability. This translation
often results in a "clunky" shoulder or one which goes "dead" when
called upon to throw at pace. Anil Kumble's shoulder had a damaged
labrum due to his high-arm legspin action. Years of repetitive stress
had detached his labrum from the glenoid, resulting in the need for
surgery. He's not alone. Muttiah Muralitharan and Shane Warne also had
shoulder surgeries in their careers. And it's not just spin bowling, as
many labral compression injuries occur during fielding when diving onto
an outstretched arm.
Injury to the cuff, however, also results in a dynamic instability,
whereby the HOH is again not held centred, and subsequently over time
stresses both the labrum and cuff. Impingement is a common term used to
describe a narrowing of the space in the shoulder that can result from
this loss of centering. The cuff doesn't actually need to be injured for
this to occur - repetitive throwing can tighten the posterior cuff
muscles and effectively "squeeze" the HOH out of its normal centre of
rotation in the glenoid. It really is a vicious circle and cricketers
compound any underlying dysfunction by the repetitive nature of the
game. They might not throw much in a match but when they do it is
usually with great speed. The bulk of the throwing volume occurs during
their practice sessions.
And when talking about shoulder mechanics we need to also understand
critical role of the scapula. In order to ensure that the HOH remains
remain centred in the glenoid, the scapula must slide and rotate
appropriately around the chest wall (that soccer ball example). Any
dysfunction in scapula movement is typically evidenced by a "winging"
motion when the arm is elevated or by observing the posture of the upper
back. Whether the winging comes before the injury or as a consequence
is hotly debated. Either way it needs to function properly. And to
complicate things even further, the thoracic spine also needs to be able
to extend and rotate fully to allow the scapula to move. Kyphotic or
slouched upper backs are terrible for allowing the arm to reach full
elevation and is a big contributor to shoulder problems.
It should be clear that in order for a cricketer's shoulder to be
pain-free, there needs to be a lot of dynamic strength and mobility of
the upper trunk and shoulder girdle. But throwing technique is equally
critical to both performance and injury prevention. Studies have shown
that the shoulder itself contributes only 25% to the release speed of
the ball. To impart this 25%, the angular velocity of the joint can
reach 7000 degrees per second. However, what is interesting is that a
whopping 50% is contributed by the hips and trunk when the player is in a
good position for the throw (allowing for a coordinated weight
transfer). But when off-balance and shying at the stumps, as often
occurs within the 30-yard circle, the shoulder alone can be called upon
to produce more than its usual load. Thus it is important to remember
that throwing should be considered as a whole body skill.
|
|||
Often a player will be able to bowl without experiencing symptoms, but
will struggle to throw. In these cases, it is common to find pathology
involving the long head of biceps or where it anchors superiorly onto
the labrum. The latter is also commonly known as a SLAP lesion. In the
transition from the cocking to acceleration phase of throwing, the
shoulder is forcefully externally rotated. The biceps is significantly
involved in stabilising the HOH at this point and often pulls so hard
that it peels the labrum off the glenoid, giving symptoms of pain and
instability. The overhead bowling action, however, does not put the
shoulder into extremes of external rotation and hence symptoms do not
usually occur. If pain is experienced during the release phase of
throwing then there is a good chance that technique is again at fault.
In order to decelerate the arm after the ball is released, the trunk and
arm need to "follow through", using the big trunk muscles and weight
shift towards the target. Failure to do this results in a massive
eccentric load on the biceps tendon, also potentially tugging on its
anchor on the glenoid. Throwing side-arm to avoid extremes of external
rotation and pain is a common sign that all is not well internally.
As you can see, an injury to the shoulder is not a simple problem. And
there are many other types of pathology found. It requires thorough
assessment and management of a host of potential contributing factors
which are mostly modifiable when identified. And whilst a lot can go
wrong in a cricketer's shoulder, there is a lot that can be done to make
sure it stays strong and healthy. Because prevention is always better
than surgery in terms of outcomes, next week I'll discuss some shoulder
training and injury prevention tips used by elite cricketers.